イントロダクション(ThermiVa誕生の背景)
外陰腟弛緩とその医療症状としての関連性については最近女性の方が医師と相談することが多くなった。
昔から婦人科症状や泌尿器科症状で困っていた女性の方が無言で我慢していたが、近年、医師に相談できるようになった。
それに応じて、医師が外陰腟弛緩の臨床的重要性を認めて治療を探している。
「Vaginal Rejuvenation」という用語が話題になり検討された。
この用語に対する一般認識は3つのカテゴリーに分けられる。
・失禁や脱出の治療
・外陰部外観の改善
・女性の性的満足度の改善
外陰腟弛緩は(腟弛緩と同じく)加齢と自然分娩に関連性がある。
以前の外陰腟弛緩とその症状の治療は骨盤底筋を強めるための効果の低い非侵襲性のケーゲル体操、または値段も侵襲性も危険度も高い手術いずれかの治療法しかなくてかなり狭い選択肢であったが、最近その間の代替治療法ができている。
そのギャップを埋めるために、腟の治療ができるレーザーまたは RF エネルギ ーを用いる機械が作られた。
美容皮膚科と形成外科で行われている顔、首、デコルテなどの治療のように、レーザーまたは RF エネルギー機器利用での外陰腟リジュべネーションはまだ新しく効果性の高いと思われる治療法である。
組織の引き締めと皮膚に傷をつけずコラーゲン産生を刺激する理想の治療温度(40°C~45°C) が多数の美容医療研究に示された。
Transcutaneous temperature controlled radiofrequency (TTCRF)という治療法の利点が多い。
コラーゲン産生の刺激、コラーゲンの変性、収縮、治癒過程の活性化によって組織を引き締めることが認められた。
レーザー治療と違ってスキンタイプ(色、または色素) は問題ではない上に、顔の皮膚に効果がも出るが、モイスチャーの高い部位の腟と外陰部にはさらに効果が高い。
温度調整式RF治療に使われるハンドピースは皮膚の温度とインピーダンスを測定してRFジェネレーターにフィードバックを提供する温度センサーが搭載されて、それに答えて、ジェネレーターがパワーを調整して治療中に設定温度を保つことができる。
利点としては、医師が選んだ設定温度にきちんと調整される RF エネルギーで治療できる。
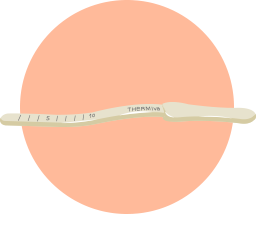
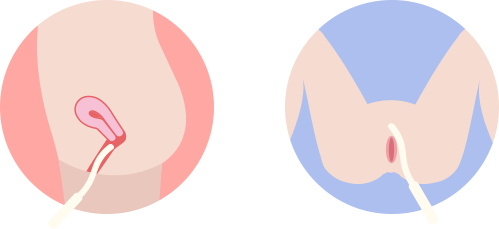
ハンドピースの活性領域のサイズは切手のサイズに近くて、ハンドピースの先の一方に搭載されている。ハンドピースの形と活性領域の位置によって治療が行ないやすい。TTCRF 治療用ハンドピースが人気で数十年婦人科に使われているのHegar dilator をイメージとして 20cm 長くて曲線の形に作られた。
TTCRF治療は治療部位を前後の動きで治療してコラーゲン産生と収縮を刺激ために皮膚を少しづつ温めて皮膚を引き締める炎症反応を起こす。
患者による冷やす必要なくとても快適な治療である。
この研究は TTCRF 治療の安全性、忍容性およびは臨床的有効性と補助的な効果を認めてもっと研究を進めることを目的としている。
材料及び方法
自己申告の一次または二次の軽度~中等度外陰腟弛緩を持っている23人の21~65歳(平均44歳)の患者(閉経期状態5人と閉経周辺期状態5人を含む)を選んだ
ほとんどの患者が二次症状を経験していた(オルガスム障害、腹圧性尿失禁、萎縮性腟炎等)。 調査開始まで5年以内の骨盤外科手術、重要な精神科的病状または精神科的病状に対する薬の内服、妊娠または調査中に妊娠の予定、最近の異常なPAP スミア、外陰病変または症状(皮膚炎、ヒトパピローマウイルス、単純ヘルペス、外陰ジストロフィー等)、または医師による危険な症状と研究結果に影響を与える症状を除外基準としている。
研究前全員の患者に同意書を確認していただいた。
研究開始時点に患者の検査と治療前の写真撮影を行った。研究が臨床オフィスで麻酔なしで行われた。
ひざを曲げ、腿を開いて、仰向けに横たわる姿勢に患者を位置決めした。患者に接地パッドを貼ってカップリングゲルを潤滑剤として使用した。準備が完了した後、皮膚の温度を40°C~45°C まで上げることを臨床エンドポイントとして、各部位(左大陰唇、右大陰唇、腟内の上下左右)を 3-5分治療して、トータル30分の治療を行った。
月1回(4-6週間に1回)の頻繁で3回までの治療コースで調査を行った。
治療後撮影と検査の上に、患者にアンケートを書いていただいた。
全員の患者に1年以降フォローアップを行った。
結果及び考察
治療中も治療後も熱傷、水疱、重大な合併症はみられなかった。
患者によるととても快適な治療で性交活動を含む日常活動を当日復活できた。
アンケートによる、全員の患者が約 50%の改善を認めた。
萎縮性腟炎を経験している患者 (5人、モイスチャーと快適の改善)、腹圧性尿失禁を経験している患者(5人、尿漏れの減少)、オルガスム障害を経験している患者(6人、感度の改善)にもかなり効果があった。腟乾燥を経験していた閉経期状態の5人と閉経周辺期状態の5人全員は潤滑剤と腟エストロゲンが不必要になったそう。オルガスムまで時間がかかった患者6人はオルガスムまでの時間が大分減ったそう。
全員の患者が治療にとても満足で周りおすすめして、また機会があれば治療するとアンケ ートを答えた。
皮膚の引き締めは初回の治療後でも見えるが数ヶ月後で効果がさらに見える。
今までの研究によって、問題が特にない場合のフォローアップは9~12ヶ月に1回の治療を行うが、今後の調査でもっと長期的にできる最適の頻繁が認められる可能性がある。
6人が1回で、8人が2回で、9人が3回で満足して、満足のエンドポイントまでの治療回数が患者によって異なることが認められた。1-2回で止めた患者がとても満足で次の治療を受ける必要性を感じなかった。腟の美容関係または医療関係の問題は婦人科や泌尿器科の医師に昔から知られてるが、女性問題の社会的受容が高くなったことによって女性の方が治療を求めるようになってきた。TTCRF 治療の安全性、簡単な使い方、高い効果、患者の満足感等から見ると、女性問題の社会的受容が少しづつ高くなるうちに、この新しい治療法が美容的にも医療的にも有効と考えられる。
結論として、TTCRF 治療は外陰腟リジュベネーションに対してとても安全で有効な治療である。
医師のカウンセリング・患者の状況にもよるが、オルガスム障害、腹圧性尿失禁、萎縮性腟炎、膀胱脱出、直腸脱出に対しての使用が勧められている。
今後とも潜在的適応を探す様々な調査が行われると強く思われる。
INTRODUCTION
The conditi on of vulvovaginal laxity and its relevance as a concerning
medical conditi on has recently become a discussion point between
women and their physicians. The att enti on and discussions
surrounding gynecological and urological issues that women face
may have historically gone by without any discussion, but thankfully
today women are openly sharing their concerns with their doctors.
In turn physicians are recognizing the clinical importance of vulvovaginal
laxity and are looking for soluti ons for their pati ents.
The term ‘vaginal rejuvenati on’ has received a lot of att enti on and
scruti ny. According to an arti cle by Lauri Romanzi, M.D. (htt p://
www.urogynics.org/2010/06/20/vaginal-rejuvenation-defined/)
public percepti on of the term seems to fall into any of three categories:
correcti on of inconti nence and prolapse, improvement in the
appearance of vulvar structures, and enhancement of female sexual
grati fi cati on.
Vulvovaginal laxity (as with vaginal laxity) is associated with advancing
age and the trauma of childbirth. Treatment of vulvovaginal laxity
and related aspects in the past lay within a short spectrum heavily
weighted at the ends. On one side stood non-invasive but minimally
eff ecti ve Kegel exercises to strengthen the pelvic fl oor, with risky,
costly, and highly invasive surgery at the other end. Only recently
have alternati ves appeared to fi ll in the center of that range.
In response to this gap, modaliti es
harnessing laser or radiofrequency
(RF) energy and others for vaginal
use have emerged. Vulvovaginal
rejuvenati on with energy based
devices, as is done in aestheti c dermatology
and plasti c surgery on the
face, neck, and decollete, is a fairly new concept with real potenti al
for success. Numerous studies in aestheti c medicine have demonstrated
ti ssue contracti on and determined a therapeuti cally ideal
temperature range (40°C to 45°C) in which neocollagenesis (via the
healing cascade) is sti mulated without causing unnecessary damage
to the skin or integral ti ssue structures.
Transcutaneous temperature controlled radiofrequency (TTCRF)
brings with it numerous advantages to treatment. It is an established
modality for ti ssue ti ghtening via sti mulati on of neocollagenesis,
denaturati on of collagen, contracti on, acti vati on of the
healing cascade. Unlike laser-based treatments skin type (color, or
pigmentati on) is not an issue with RF energy, and while it is showing
consitent positi ve results when used for surface skin on the face
and other areas of the body, RF energy is even more eff ecti ve in
ti ssue that is naturally moist and well hydrated, as seen with vaginal
and labial ti ssue. The RF electrode used in temperature controlledprocedures have a temperature sensor located at the ti p; the thermocouple
measures ti ssue temperature and and impedance, which
provides feedback to the RF Generator; in turn the generator will
adjust the power allowing the device to maintain a given set temperature
throughout the treatment. The benefi t is the physician can,
for the fi rst ti me, treat using precisely controlled RF energy at a preselected
temperature setti ng.
The RF electrode has a treatment
acti ve area of the size similar to
a postage stamp. This acti ve part
of the electrode rests within one
side of the electrode close to the
ti p. The form of the electrode
and locati on of the acti ve treatment
ti p allows for easy placement on targeted ti ssue. The TTCRF
treatment electrode is about 8 inches long with a slight ‘S’ curve at
center, patt erned aft er the highly successful Hegar dilator that has
been in gynecologic use for decades. During TTCRF the RF electrode
is passed back and forth over the desired area unti l the ti ssue is
gradually heated to the therapeuti cally relevant level to induce collagen,
shrinkage and create an infl ammatory response which results
in neocollagenesis, and its eff ect of ti ssue ti ghtening. Pati ents report
comfort during the procedure with no need for external cooling.
The purpose of the study is to evaluate the safety, tolerability and
clinical effi cacy of TTCRF as well as anecdotally document possible
ancillary benefi cial eff ects of treatment, to promote further study.
MATERIALS AND METHODS
Subjects (n=23; age range 21-65 years, mean 44; 5 menopausal, 5
perimenopausal) presented with self-described mild to moderate
primary or secondary vulvovaginal laxity. Associated secondary conditi
ons (orgasmic dysfuncti on, stress inconti nence, atrophic vaginiti
s, etc.) were present in most subjects. Exclusion criteria included
pelvic surgery less than 5 years from the beginning of study, presence
of major psychiatric conditi ons or related need for medicati on,
pregnancy or planned pregnancy within the study period, recent abnormal
Papnicolaou test result, presence of vulvar lesions or disease
(dermati ti s, human papillomavirus, herpes simplex, vulvar dystrophy,
etc.), or the presence of any conditi on or circumstance that, in
the opinion of the investi gati ng physician, may be unsafe or otherwise
interfere with the study. Informed consent was obtained from
all subjects prior to commencement of the study. Pre-treatment
digital photography was performed at baseline along with physician
evaluati on of pati ents. Treatment was performed in a clinical offi ce
setti ng and no anesthesia was required. During treatment subjects
were placed on a treatment table in the dorsal lithotomy positi on.
A neutral return electrode pad was placed on the subject, with a
coupling fl uid used as a lubricant for treatment with the ThermiVa
TTCRF TM device (ThermiGyn, SouthLake, TX). Once pati ents were
sett led and comfortable they were treated using the TTCRF device
for 3-5 minutes per zone: the left and right labia majora, and the
ventral, dorsal, left and right surfaces of the vaginal wall. Clinical
endpoint was achievement of the target temperature in the range
of 40°C to 45°C. Total treatment ti me was less than 30 minutes. A
complete course of therapy consisted up to three treatments with
the TTCRF device, at an interval of approximately one month (4-6
weeks).
In additi on to photography and physician evaluati on, pati ents completed
a questi onnaire about their experience, treatment comfort
and sati sfacti on with results.
Follow-up occurred for at least one year for all subjects.
RESULTS AND DISCUSSION
There were no burns, blisters or major complicati ons during and after
treatments, which were described as pleasant and very comfortable.
Pati ents were able to resume all acti vity, including sexual intercourse,
as normal immediately aft er each treatment. All pati ents
saw signifi cant improvement, averaging 50%; measurable changes
were revealed via pati ent questi onnaire. Notable improvement was
also seen in cases including atrophic vaginiti s (n=5, improved moistness
and comfort), stress urinary inconti nence (n=5, noti ceable
reducti ons in leakage), and orgasmic dysfuncti on (n=6, noti ceable
improvement reported). Of the perimenopausal (5) and menopausal
(5) pati ents who had complaints of vaginal dryness prior to treatments,
all were able to eliminate the need for lubricant use and vaginal
estrogens. Six women who had diffi culti es in achieving orgasms
reported that the ti me to orgasm was dramati cally shortened. All
pati ents were happy or very happy about the treatment and results,
and would both undergo it again and recommend treatment to
others. Some ti ghtening result is visible immediately aft er the fi rst
treatment but the full outcome takes a few months to fully manifest.
The course of follow-up from one year and beyond revealed that
outcomes last 9 to 12 months before a touch-up is required, so pa-ti ent can expect to need an additi onal maintenance session once
or twice a year; additi onal study with larger populati ons examining
protocol refi nements may reveal more ideal treatment parameters
and further delineate persistence of outcomes. It is interesti ng to
note that 6 pati ents received only one treatment, 8 pati ents completed
two treatments, and 9 received a third treatment to reach
a sati sfactory endpoint. The pati ents who dropped out early were
extremely happy with their results aft er only one or two treatments
feeling that it was not necessary because they had achieved all of
their endpoints.
While the variety of possible medical and aestheti c concerns associated
with the vagina and related structures are not novel to gynecologists
and urologists, increasing social acceptance of the vagina and
reference to it have not only shed additi onal light on the prevalence,
but will conti nue to boost demand for therapies addressing those
issues. This is a boon to pati ents otherwise left to their own devices.
Given the safety, simplicity and ease of treatment associated with
TTCRF as well as the remarkable results and high pati ent sati sfacti on
with virtually no risk, downti me, or discomfort, this novel therapy
shows much promise in both the medical and aestheti c arenas in an
increasingly accepti ng social climate.
In conclusion, TTCRF for vulvovaginal rejuvenati on is safe, tolerable
and eff ecti ve for vulvovaginal rejuvenati on. Evidence strongly suggests
applicati ons in the treatment of atrophic vaginiti s, orgasmic
dysfuncti on, stress inconti nence, and prolapse of the bladder or rectum.
Further investi gati on via randomized, controlled trials isolati ng
and exploring various potenti al indicati ons is more than warranted.